EMT-6 Syngeneic乳腺肿瘤模型 - 一种强大的免疫肿瘤学研究工具
AUTHOR:
谢Barnes博士|导演,三英洁具tific Development
日期:
2018年5月
乳腺癌是美国女性中最常见的癌症,是癌症死亡的第四个主要原因。在2017年,估计诊断出252,710例新病例(占所有新癌症的15%)和40,610名患者死亡。早期检测举措与改善的治疗方案一起导致5年的整体生存率增加到1975年的75%至超过90%。[1]尽管存在有利的存活统计,转移性疾病仍然是治疗挑战,并且经常导致死亡。因此,需要持续开发乳腺癌新治疗方法。
Advancements in Using Immuno-oncology Combination Therapies for Breast Cancer
While several treatment options are available to fight hormone- or Her2-driven breast cancers, options are somewhat limited for三重阴性乳腺癌不能利用这些有针对性的疗法的患者。添加到这个问题,尽管在治疗黑素瘤和肺癌中的免疫治疗方面取得了成功,但乳腺癌已被证明是特别难以检查点封闭或其他免疫治疗。然而,近年来的重点努力免疫肿瘤学乳腺癌接近,新兴临床数据显示有望,特别是在联合治疗中。[2]为了帮助推动这项研究,Covance已经开发了EMT-6 Syngeenic乳腺肿瘤模型。来自Balb / C小鼠中的移植的增生肺泡结节衍生,[3]该模型利用完整的小鼠免疫系统,并用作免疫肿瘤间空间中的强大工具。
使用EMT-6模型测试组合疗法
AUTHOR:
谢Barnes博士|导演,三英洁具tific Development
日期:
2018年5月
乳腺癌是美国女性中最常见的癌症,是癌症死亡的第四个主要原因。在2017年,估计诊断出252,710例新病例(占所有新癌症的15%)和40,610名患者死亡。早期检测举措与改善的治疗方案一起导致5年的整体生存率增加到1975年的75%至超过90%。[1]尽管存在有利的存活统计,转移性疾病仍然是治疗挑战,并且经常导致死亡。因此,需要持续开发乳腺癌新治疗方法。
Advancements in Using Immuno-oncology Combination Therapies for Breast Cancer
While several treatment options are available to fight hormone- or Her2-driven breast cancers, options are somewhat limited for三重阴性乳腺癌不能利用这些有针对性的疗法的患者。添加到这个问题,尽管在治疗黑素瘤和肺癌中的免疫治疗方面取得了成功,但乳腺癌已被证明是特别难以检查点封闭或其他免疫治疗。然而,近年来的重点努力免疫肿瘤学乳腺癌接近,新兴临床数据显示有望,特别是在联合治疗中。[2]为了帮助推动这项研究,Covance已经开发了EMT-6 Syngeenic乳腺肿瘤模型。来自Balb / C小鼠中的移植的增生肺泡结节衍生,[3]该模型利用完整的小鼠免疫系统,并用作免疫肿瘤间空间中的强大工具。
使用EMT-6模型测试组合疗法
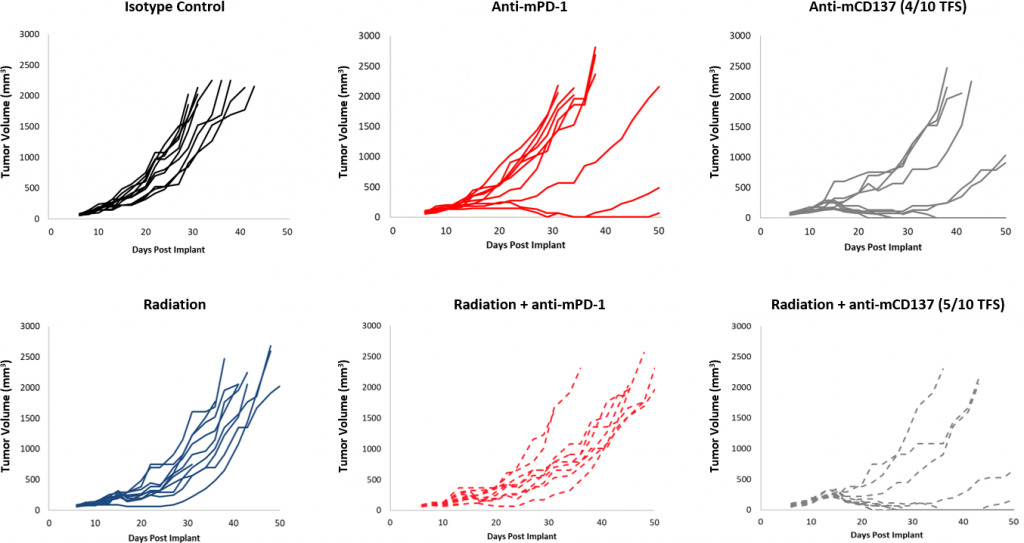
In this spotlight, we present data from our initial efficacy study with the EMT-6 model. These data should enable the design of rational combination studies with novel therapeutics while additional studies are performed. Control tumor growth for the EMT-6 model is shown in Figure 1. The median doubling time is 5.5 days on average, allowing for a therapeutic window of at least three weeks with which to elicit anti-tumor activity. The growth rates of untreated tumors and those treated with an isotype control antibody (rat IgG2b) are nearly superimposable. To determine the response of EMT-6 to immunomodulatory therapies, mice bearing EMT-6 tumors were treated with checkpoint blockade (anti-mPD-1 and anti-mPD-L1), and anti-mCD137, a costimulatory molecule. Additionally, as focal radiation is oftentimes used to treat breast cancer, we included modeling of radiation monotherapy and combination therapy.

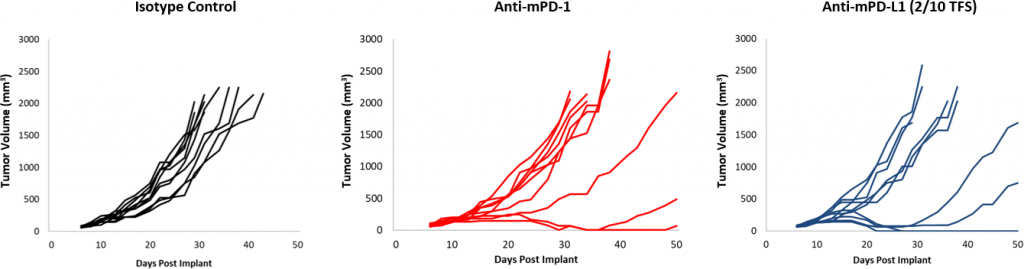
与对照相比,对检查点封闭的反应是适中的(图2)。虽然动物的子集确实响应,但用抗MPD-1和抗MPD-L1治疗仍然为组合提供改善的空间。此外,Afocal radiationdose of 10Gy, which causes significant tumor growth delay in other syngeneic models, offered only modest activity in EMT-6. Addition of anti-mPD-1 to this regimen offers some additive impact, yet still leaves room for improvement in triple combination. In contrast, treatment with anti-mCD137 monotherapy results in a strong response (4/10 TFS) against EMT-6. Combination with focal radiation offered nominal improvement (5/10 TFS) over anti-mCD137 monotherapy (Figure 3). These data demonstrate the advantage of using the EMT-6 model to investigate dual or triple combination strategies which utilize radiation, checkpoint blockade, and/or costimulatory molecule agonists.
Composition of Infiltrated Immune Cells Within the Tumor
当询问免疫脑神经理目的时,将渗透的免疫细胞的组成变为肿瘤也很重要。为此,检查220-385mm 3之间的肿瘤,用于渗透到T细胞,骨髓细胞表达为CD45 +细胞的百分比(图4)。所有肿瘤上的骨髓隔室均匀地分布在M2巨噬细胞,单核细胞MDSC和粒细胞MDSC上。M1巨噬细胞渗透比其他骨髓衍生细胞相对较低。该组合物提示免疫抑制微环境,这有助于解释测试的大多数免疫疗法方案的有限反应。
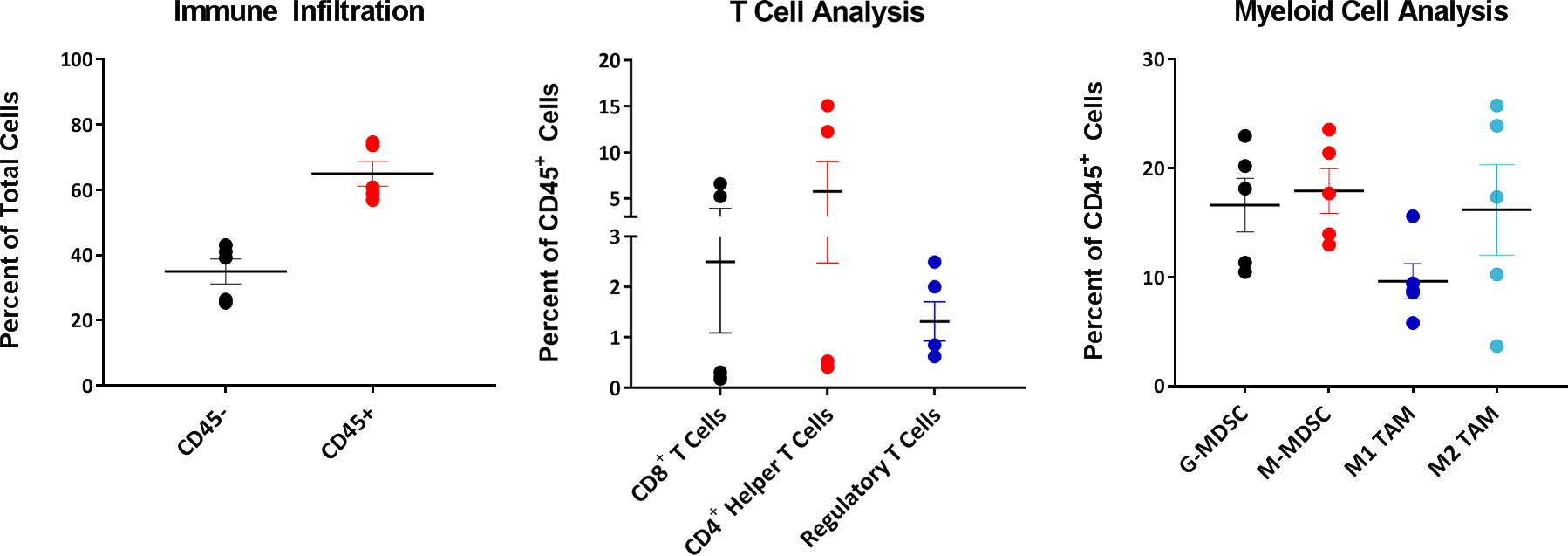
相比之下,T细胞隔室显示出间间变异性,其中三种肿瘤中的三种肿瘤显示出很低的CD4+和CD8+T cells. Interestingly, the Treg composition in these tumors exhibited much less variability between tumors when compared to CD4+和CD8+T细胞渗透。正在进行研究以确定用渗透的CD4看到的可变性+和CD8+T cells across these EMT-6 tumors is inherent to the biology of this model or if variability would normalize given a larger sample size.
EMT-6 – A Robust Preclinical Immuno-Oncology Model
EMT-6同系乳腺癌模型具有良好的免疫曲线,可用作稳健的临床前免疫脑肿瘤模型。yaboapp体育官网我们的数据支持使用该工具在调查具有辐射,检查点抑制剂或共刺激分子的新型治疗组合。请联系人与我们的科学家们谈论EMT-6或我们的其他一体的模型,可用于您的下一个免疫肿瘤学研究。
模型聚光灯|EMT-6 Syngeneic乳腺肿瘤模型 - 一种强大的免疫肿瘤学研究工具(PDF版)
[1]Howlader N,Noone Am,Krapcho M,Miller D,Bishop K,Kosary Cl,Yu M,Ruhl J,Tatalovich Z,Mariotto A,Lewis Dr,Chen Hs,Feuer EJ,Cronin Ka(EDS)。SEER癌症统计审查,1975 - 2014年,国家癌症研究所。Bethesda,MD,https://seer.cancer.gov/csr/1975_2014/,基于2016年11月的Seer数据提交,发布到Seer网站,2017年4月。[2]Vonderheide,Rh,Domchek Sm,Clark,As(2017)乳腺癌免疫疗法:我们错过了什么?Clin Cancer Res,23:2640-2646。[3]Rockwell SC,Kallman,RF,Fajardo,LF(1972)的连续移植的小鼠乳腺肿瘤特征及其组织培养适应衍生物JNCI,49:735-749。
注意:研究是根据AAALAC认可的设施中适用的动物福利法规进行的